
Innovative Strategies in Disease Prevention: Introducing SPRC’s New Faculty
#Interventions
One of the past year’s most exciting developments for the Stanford Prevention Research Center (SPRC) was adding three distinguished new faculty to its roster of prominent experts in preventive research.
“Almost all our faculty were full professors. We needed new perspectives, new blood. That’s what prompted us to bring on these three brilliant, successful scientists with tremendous potential who bring their own methods to prevent common chronic diseases,” says SPRC Chief David Maron, MD, the C.F. Rehnborg Professor of Medicine.
The three new faculty are:
- Shoa Clarke, MD, PhD, assistant professor of cardiovascular medicine and of pediatrics, who is seeking to improve genetic risk prediction for coronary artery disease in Black and Hispanic populations.
- Lisa Henriksen, PhD, associate professor of medicine, who is leading a research program about tobacco and cannabis, with the goal to inform state and local policy interventions.
- Alex Sandhu, MD, assistant professor of cardiovascular medicine, who notes that coronary artery calcium is probably the strongest risk predictor for who will have a heart attack or stroke.
“We’re all trying to better understand how we can prevent disease morbidity everywhere along the spectrum. At one end, we’re trying to prevent healthy people from developing initial disease. At the other end, we’re aiming to stop people who already have had heart failure from developing other health problems,” says Sandhu, a cardiologist who specializes in heart failure. “But we’re obviously targeting that from such very different perspectives and different levels of intervention.”
From Henricksen’s research about tobacco and cannabis to Clarke’s work in bridging genomics and bioinformatics to Sandhu’s efforts to narrow the gap between evidence and practice in the treatment of heart disease, the new faculty shared more about their unique backgrounds and interests, what brought them to the SPRC, and their current research.
How did you get into this work?
Clarke:
I was a student at Stanford under the MD-PhD Program and focused my PhD activities on nonclinical research related to genomics and bioinformatics. After learning how to do computational work with very large data, I wanted to apply those skills to medicine. I was fascinated by the notion that we carry our genome with us from birth to death, which led me to do an unusual residency that combined both internal medicine and pediatrics. During my residency, I first encountered patients with a genetic disease called familial hypercholesterolemia, and that was my inspiration for how I could apply my skill set.
Henriksen:
As a doctoral student in communication and developmental psychology at Stanford, I enjoyed an early experience with the talented researchers at SPRC. I collaborated with an investigator leading a longitudinal study of third, fifth, and seventh graders about risk factors for early initiation of tobacco and alcohol use, with implications for parenting recommendations. But my current work focuses on systems-level (policy) implications instead.
Sandhu:
I wanted to get additional training in the methodology of clinical research and health economics. That led me to pursue a master’s in health policy research, where I worked very closely under [Professor of Cardiovascular Medicine] Paul Heidenreich on cost-effectiveness and policy: how we can deliver higher value care. Then, later during a heart failure fellowship, my focus shifted from health economics and health policy to implementation – actually delivering care strategies at the point of care.
What led to your current appointment?
Clarke:
I was hired at SPRC for two reasons. Our chief [David Maron] wanted to gain more clinical expertise in the division and was seeking someone who practices preventive cardiology, which is what I do in my clinical practice. I was also brought on because of my research, which is focused on the genetics of cardiovascular diseases and the idea that we may be able to use genetics and potentially other factors to better predict who’s at risk of early heart attacks.
Henriksen:
I was promoted to associate professor at SPRC to lead a research program about tobacco and cannabis, the latter being widely available in tobacco shops. The main focus of my research is to inform state and local policy interventions. I am principal investigator of Advancing Science and Practice in the Retail Environment – ASPIRE, one of four program projects in the Department of Medicine funded by the National Institutes of Health (NIH). I also led an NIH-funded study about cannabis and other drugs in the tobacco retail environment.
Sandhu:
The central premise behind my work and how it aligns with the Stanford Prevention Research Center is that we have incredible interventions in the cardiovascular space to prevent the massive morbidity of cardiovascular disease. But there are huge gaps between evidence and practice – doing what we know works across the population. My research seeks to better understand those gaps and then test novel strategies to reduce them.
What are some highlights of your current work?
Clarke:
I currently have funding through Stanford’s K12 career development program for work aimed at improving genetic risk prediction for coronary artery disease in Black and Hispanic populations. Another research endeavor involves the use of longitudinal data that are now available in electronic health records to go beyond genetics to predict who might be at risk of disease. And then I have two clinics – a preventive cardiology clinic on the adult side and also one at Lucile Packard Children’s Hospital Stanford. So I see both adults and children who are potentially at high risk for developing cardiovascular disease, including familial hypercholesterolemia.
Henriksen:
My research shows that Black residents in the United States are disproportionately exposed to lower prices and more advertising for menthol cigarettes. The results provide evidence of why the impending rule on banning menthol cigarettes is so important. Beyond marketing, my research is also concerned with place-based differences in the concentration of tobacco retailers in neighborhoods characterized by economic disadvantage and a high proportion of racially/ethnically minoritized residents. The goal of this work is to inform policy interventions.
Sandhu:
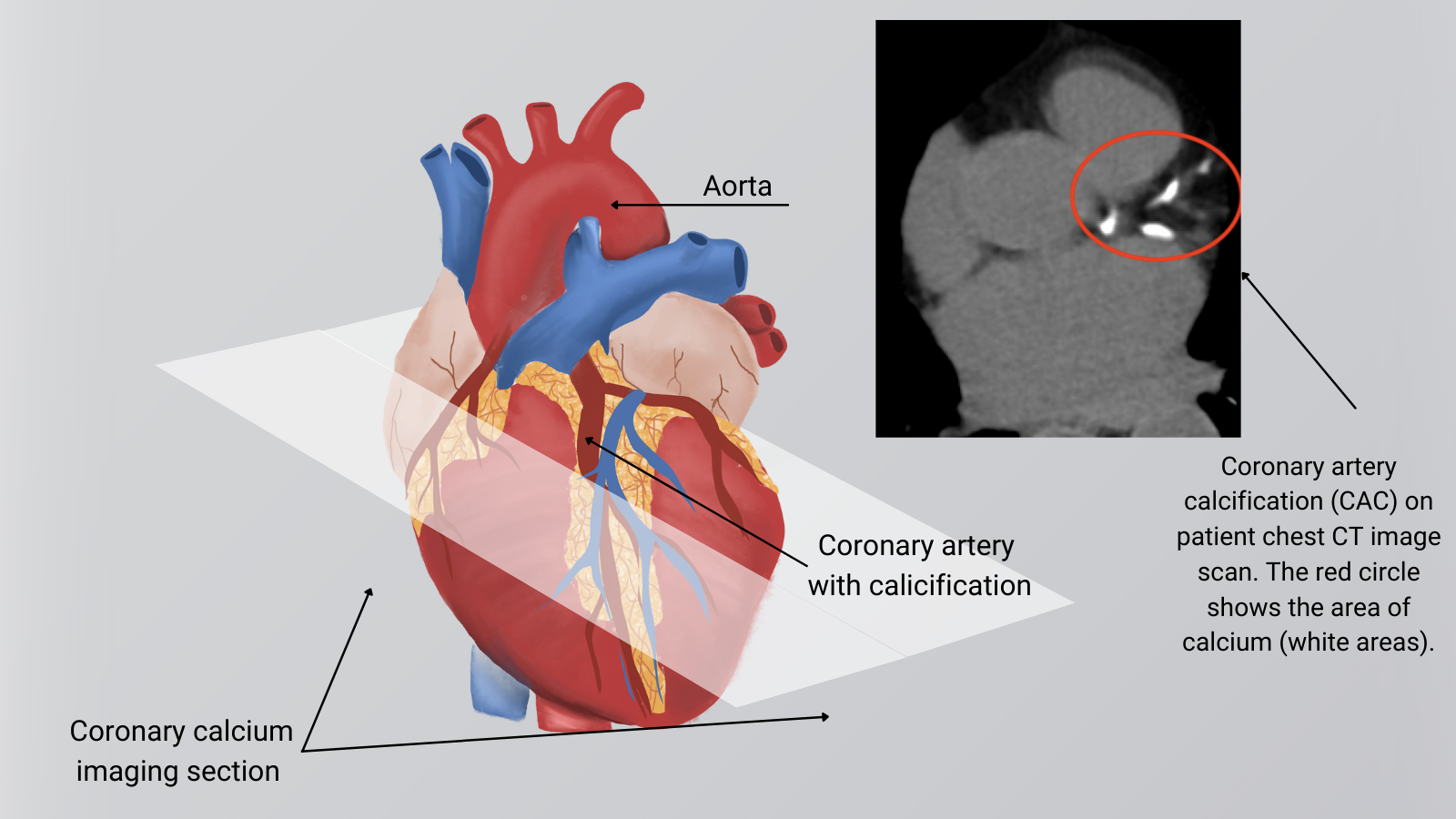
Coronary artery calcium (CAC) is probably the strongest risk predictor for who will have a heart attack or stroke. In our NOTIFY-1 (Incidental Coronary Calcification Quality Improvement) project, we worked with computer scientists at Stanford to develop an algorithm to quantify the amount of CAC based on chest CTs. That algorithm led to a quality improvement project in the Stanford Health Care system and is now used in more than 50 hospitals nationwide. In addition, we used pictures from patients’ chest CTs with coronary calcium circled to urge those patients to discuss that finding with their primary care clinician. That led about half of them to start on a statin medication to lower their risk of heart attack or stroke. By comparison, only 7% in a similar group that was not notified started on a statin, so that shows how we can leverage data science to motivate patients to practice preventive health. View image of coronary artery calcification.
{kind=link}